Use this toolkit alongside the improvement science guide for a step-by-step explanation and the tools you need at each stage.
Use this toolkit to plan, run and sustain a medication reconciliation quality improvement project. It includes worked examples, templates and resources you can adapt to your local setting.
Register to gain access to the Community of Practice in the Improvement project section of the Quality Improvement Data System (QIDS). Available to NSW Health staff only.
Getting started
It is important to set a realistic timeline before starting a QI project. Improvements usually take 12 to 18 months to initiate, test, embed and sustain. The timeline may be shorter if your team has done similar improvement work before. It may be longer if the change is complex or involves multiple services and departments.
Start by identifying a specific Med Rec problem at your facility. Common examples include:
- low completion rate of admission Med Rec on a clinical unit or ward
- poor documentation of best possible medication history (BPMH)
- inaccurate transfer of medicines information at transfer of care.
At this stage, name the problem only. Do not propose solutions yet.
People and teams do not always welcome change, even when the goal is improvement. Resistance from those most affected can stall a project's momentum. See Improving practice and culture for ways to manage this.
Use the Med Rec readiness assessment tool (PDF 205.8 KB) to identify practical changes for your service.
Improvement projects need a problem that people are motivated to solve. Common errors at this stage include:
- selecting a problem no one is interested in
- jumping to a solution before investigating the problem
- focusing on a process that is currently unstable (for example, a paper-to-electronic transition)
- choosing a problem outside your team's sphere of influence.
Assess your unit's readiness for change by reviewing existing culture, communication, team practices and safety and quality concerns. If there is significant resistance, address it before proceeding.
More about Improving practice and culture
Gather local data to support the problem you have identified, using sources such as:
- eMeds reports on Cerner sites: EM002 (Meds Rec Compliance Audit), EM003 (Meds Rec Current Inpatients), EM007 (Medication History Audit)
- incident management system data (ims+, Incident Information Management System (IIMS))
- pharmacy intervention progress notes
- baseline audit of medical records (around 20 randomly selected records, distributed evenly across wards)
- staff and patient stories about how poor Med Rec has affected care.
- gap analysis of each Med Rec process task to show current state versus target state, so improvement can focus on one or two tasks or the areas of greatest need (see Med Rec gap analysis (PDF 235.5 KB) for more information)
- literature search: conduct literature reviews.
Seek guidance from your clinical governance unit, infectious diseases, pharmacy or infection control departments. You can also contact us for advice on sampling numbers and data sources.
The improvement project brief sets out the problem, why it matters, how long the work will take and the approach you will use. A strong brief is grounded in your data, takes sustainability into account, and aligns with your health service's priorities.
Your brief should include:
- why Med Rec is important, with supporting evidence
- what the problem is, with data
- the changes you want to make and their expected benefits
- how the project aligns with your organisation's plan and priorities
- the support and resources required
- a realistic timeline.
Use the brief to gain a project sponsor, someone in a senior position, ideally not working directly on the project, who has authority to remove barriers and secure resources. Communicate with your sponsor regularly.
Download Med Rec improvement project brief template (PDF 16.3 KB) to build your case.
Find a project sponsor early. Present your case for change and ask them to support the work.
A good sponsor:
- has authority to approve changes
- secures the resources the team needs
- helps remove barriers as they arise
- holds a senior role but does not work directly on the project
- believes the problem is worth solving
Communicate closely with your sponsor and provide regular updates.
Use the Med Rec improvement project brief (PDF 16.3 KB) to brief your sponsor and project team.
Your project sponsor can guide where governance sits within your health service. Operational responsibility usually integrates with existing meetings:
- Unit or ward level: Quality use of medicines review meetings or departmental meetings.
- Health service, local health district or speciality health network level: Drug and therapeutics committee or medication safety committee meetings.
Governance is separate from your project team. The project team carries out the interventions.
Where to get help
Contact your clinical governance unit to connect with local QI experts, the drug and therapeutics committee, medication safety committee, or quality use of medicines review meetings. You can also reach out to colleagues in other health services about their Med Rec improvement work. For example, hospital executive, medication safety committee members, Med Rec working group or QI advisors in the clinical governance or patient safety unit.
A Med Rec project needs a multidisciplinary team with a team leader to steer it, and members committed to actively supporting it. QI projects often fail when team members lose interest or stop participating, leaving the leader to carry the work alone.
The project team's role is to:
- evaluate current medication reconciliation processes
- identify and enlist clinical champions
- set general goals
- develop, run and evaluate improvement strategies
- share results and findings.
Suggested team members
The core team includes a project lead, executive sponsor, clinical champion, and representatives from nursing, pharmacy and consumers. Depending on the scope of your project, also consider including:
- junior medical officer, emergency department physician or geriatrician
- nurse unit manager, clinical nurse consultant or clinical nurse educator
- emergency department, aged care or discharge liaison pharmacist
- discharge planner, quality and safety manager, patient safety representative.
Download the Guide to engaging a multidisciplinary team (PDF 159.9 KB)
Once the team is in place, align on the problem the project is targeting and what is in and out of scope. Without a well-defined scope, projects tend to grow beyond what is achievable, lose focus, and fail.
Making improvements
This stage moves your project from problem-definition into structured testing: writing an aim, mapping the current process, generating change ideas, and testing them in small cycles.
Your aim statement captures the goal of the project. It must address the problem and must not include a solution.
A SMART aim is specific, measurable, achievable, relevant and time bound. Remember:
- "some" or "better" is not a measure, and "soon" is not a time frame
- start small. Focus on a single unit or ward, even if the problem is widespread. Refining your approach on one unit gives you the evidence and confidence to spread the work
- avoid aim statements that suggest the desired solution, for example "implement a specific policy or process on your ward".
Examples:
- Within six months, 85% of emergency department patients on Ward 3B will have admission medication reconciliation completed within two business days of admission.
- By [month, year], 90% of discharged patients on Ward 3B will have discharge medication reconciliation completed prior to discharge.
Resources
Develop a flow chart of your current Med Rec process, from patient arrival to discharge handover. The flowchart shows how the process happens, not how it should. Pay attention to handover points between medical, nursing and pharmacy teams, after-hours and weekend processes, emergency department admissions, transfers between wards, and discharge medication supply and counselling.
Once the flow chart is agreed, analyse it as a team. Compare your current practice with the recommended Med Rec process and consider where it can be improved. See Med Rec for definitions, guidance on roles and responsibilities, and the local operating procedure.
Ask:
- What can go wrong within each step?
- How much error correction or rework is happening?
- Are you doing the right things?
- Are you doing them in the right order?
- Are the right people doing the work?
- Does the process produce the results you want?
- Is the process cost and time effective?
Identify the areas where you need data to better understand the process and its current reliability.
Once you have identified gaps with baseline data, brainstorm why they exist. Without understanding all the causes, solutions may focus on the wrong part of the process and the problem continues. Use the 5Ws and 1H brainstorm method against the gaps in your flowchart.
Brainstorming examples:
- Lack of understanding of the benefits and skills to complete Best Possible Medication History and Med Rec
- Poor stakeholder and executive engagement to support change
- Lack of standardised process and guidelines on roles, responsibilities and delegation
Resources
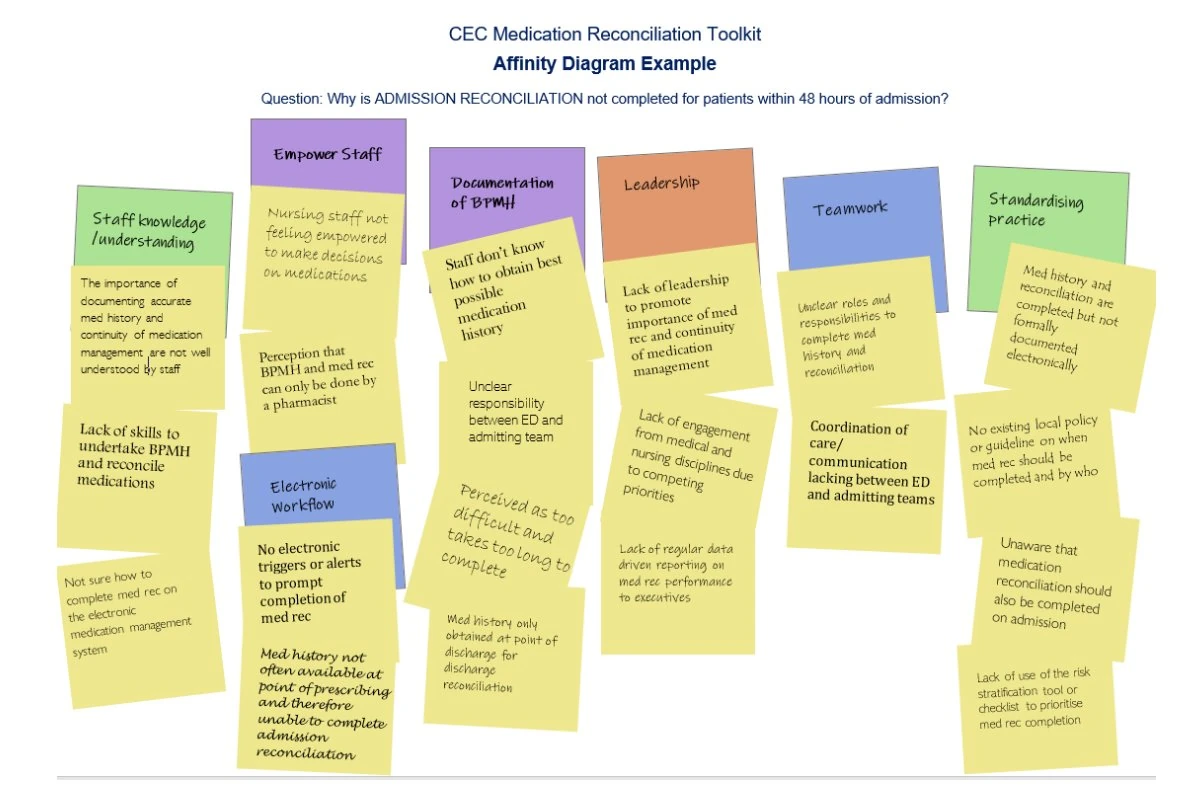
Use brainstorming, an affinity diagram, and a driver diagram to work from identified problems in the flow chart to structured change ideas. Then test change ideas using Plan, Do, Study, Act cycles. Start small (one patient, one shift, one team) and scale up as evidence builds.
Be specific when brainstorming causes. Rather than "medication history not taken on admission," try: "BPMH not completed for patients admitted overnight because pharmacy hours are 9 to 5."
Examples
- Affinity diagram example
- Affinity diagram example (NSW Health staff only)
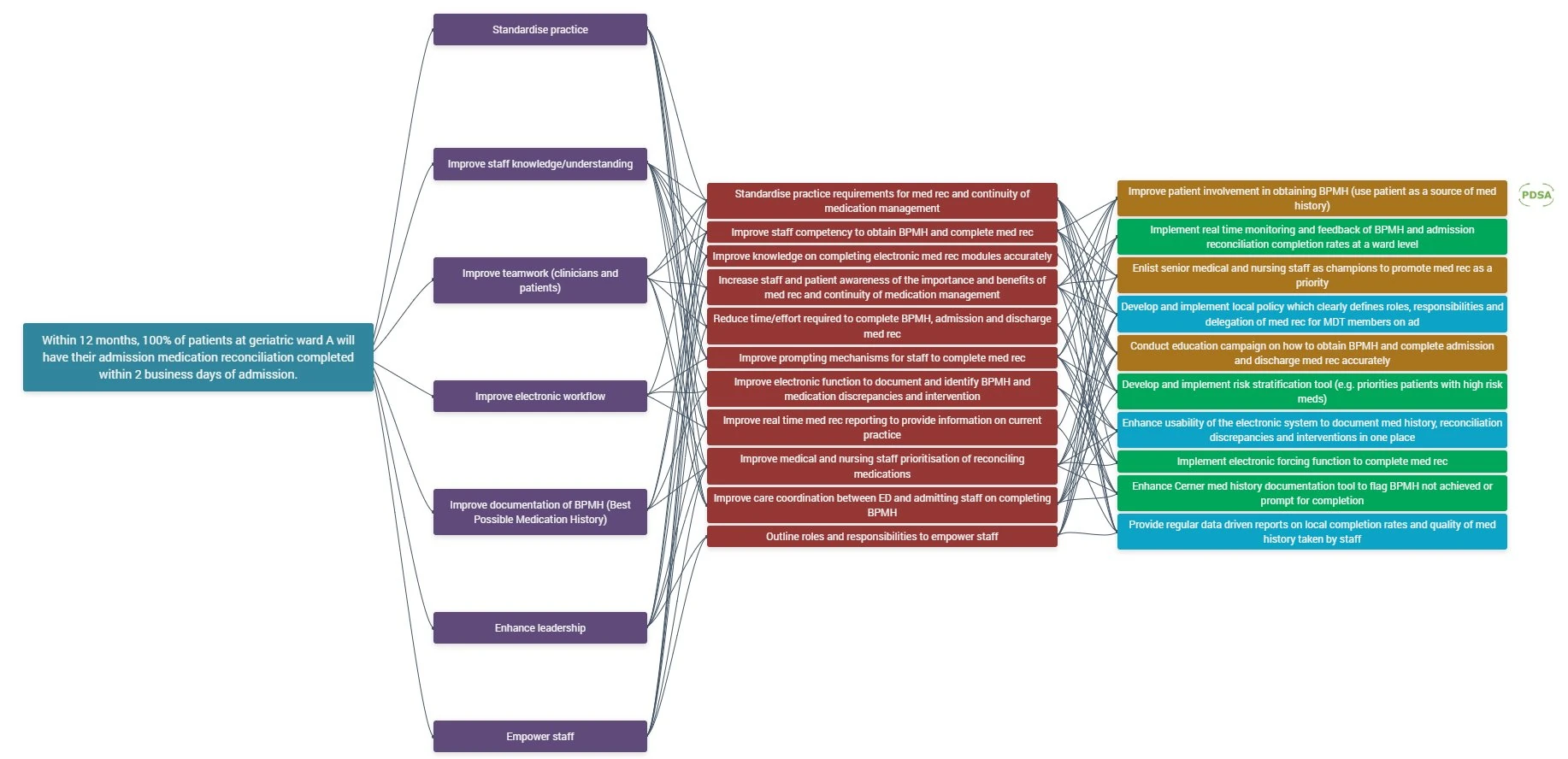
- Driver diagram with change ideas example
- Driver diagram with change ideas example (NSW Health staff only)
- PDSA example (NSW Health staff only)
- Change ideas example (NSW Health staff only)
{kind=link}
{kind=link}
Resources
Plan, Do, Study, Act (PDSA) cycles test changes on a small scale before scaling up. Start with one patient, one shift or one team. If the test works, expand (for example, three patients, three shifts, three teams), then continue scaling up.
PDSA cycles are designed to be rapid and sequential. Implementation only happens once small-scale tests achieve a reliable improvement.
Tips for PDSA cycles:
- Test no more than three change ideas at a time
- Consider testing the next change idea when the project team is confident in the first change idea (that is, starting to scale up the testing)
- Not designed to be time consuming and can be performed rapidly and in a staggered approach
- Monitor the data and measures to track improvements
- Determine which changes (or combination of change ideas) are leading to an improvement and achieving the project aim.
Data for improvement
When testing your change ideas with PDSA cycles, you will need to start collecting data to be able to determine if the changes made have resulted in an improvement. This data should be collected in 'real time' rather than retrospectively.
Download Med Rec measurement strategy template (DOC 31.1 KB)
Choose your measures
A single measure is rarely enough to determine whether improvement has happened. It is important to define the numerator and denominator and provide an operational definition for each measure to ensure data consistency.
Include one or two measures from each of three family of measures.
See measurement examples (NSW Health staff only)
Outcome measures outline the overall result you are trying to achieve. They relate to how the overall process or system is performing. In other words, the end result.
Example: completion rate of admission Med Rec within two business days of admission.
- Numerator: Number of patients with admission Med Rec completed within two business days
- Denominator: Total number of patients admitted to the ward for more than two business days
- Operational definition: Admission Med Rec completed within two business days (including BPMH). Completion is indicated by the green tick on the Cerner eMeds admission Med Rec module.
- Data source: Cerner eMeds report (EM002)
Process measures outline whether the steps in the process are working as planned. They are logically linked to achieve the intended outcome or aim.
Example: percentage of medical officers trained on completing a BPMH, taken from the education attendance sheet.
Balancing measures look at the system from different directions or dimensions. Whether changes in one area are creating problems elsewhere.
Example: rate of patients who did not receive discharge counselling from a pharmacist.
Before starting PDSA cycles, your team should:
- review any baseline or historical data on the process you want to improve
- decide if you need to collect baseline data to measure the project's impact
- agree what to measure: how, who, when and where data will be collected for each measure
- find the most efficient way to access and collect the data
- consider how useful the data will be and how you will present it (don't collect data you won't use)
- speak with staff and patients about their experiences during testing
- choose where to record data and how the team will access it (for example, a spreadsheet, or QIDS, which is preferred)
- assign responsibility for data collection to specific team members for each measure
- plan to keep collecting data after the project to check the improvements last.
The key is not quantity. Make sure the data is project-specific and can be collected continuously. Speak with your quality improvement advisor if you are unsure.
For example, if you are auditing progress notes manually, audit five random patients per week. If you are pulling data from an eMeds report, you can collect 6 to 12 months of consecutive data.
Who can help with data collection
Contact data experts or colleagues who can advise on what to collect and how much. They may already have the data you need:
- health information data team
- ICT or eMeds team
- local clinical governance or patient safety team
- medical records
- pharmacy department
- executive sponsor.
Once your team is confident a change is producing reliable improvement, implement it across the project scope.
Once data is collected, your team needs to interpret it to see if improvement has happened. Enter data into a spreadsheet or QIDS. QIDS builds charts directly from your data.
Run charts are line graphs showing data over time. They are an effective way to tell the project story and communicate progress to stakeholders. Annotate run charts to show when each change idea was tested and how it may have driven improvement. Your local QI advisor can help with displaying and analysing data.
To know if an improvement is real and lasting, look at patterns in your data over time. Probability-based rules help separate genuine change from random variation. On a run chart, for example, six consecutive data points above 95% signal a reliable improvement. This means the new process is followed 95% of the time.
See Safety intelligence data tools for more options to present data, including histograms and control charts.
Resources
Communicating change
Each group affected by your Med Rec project will need different communication approaches. The groups include medical officers, nursing staff, pharmacists, allied health, executives, patients, and project sponsors. A stakeholder engagement plan (PDF 25.9 KB) sets out who you need to reach, how often, and through what channels.
Think about how best to reach each group. Some ideas:
- use hospital-wide communication channels such as newsletters and the intranet
- engage local nursing, medical, pharmacy and Med Rec or Med Safety champions to advocate for improvement and support clinicians on the floor
- set up a ward display board or fact sheet with project information and data
- add a standing agenda item or short presentation to regular meetings
- give short, regular updates during handovers and staff meetings
- create posters, lanyards and computer screensavers (see the resources section in the top-right panel)
- hold a project launch or workshop, or fold engagement into existing events like medication safety forums and grand rounds
- run a quiz, post on social media, or send email updates
- send information to general practitioners and visiting medical officers in rural and regional areas.
Providing education
Developing and delivering education is a fundamental component to ensuring project success. Education and training will need to be delivered to a variety of stakeholder groups at numerous points throughout the project lifecycle.
- Open with an interactive poll or pre and post quiz to check perception and knowledge.
- Invite a local clinical champion to speak to the ward or unit.
- Work through a Med Rec case study or include a patient story to build engagement such as a geriatric patient with polypharmacy admitted overnight, or a mental health patient ready for discharge with multiple medication changes.
- Keep sessions short and frequent; plan coverage for staff working after hours or on weekends.
- Collect attendance records and post-session feedback to improve future sessions.
- Share planning and delivery across the team, so no one person has to do it all.
- How soon should a Best Possible Medication History be completed?
- What are the common pitfalls when collecting a medication history?
- Who is responsible for completing Med Rec at each transition of care?
Read the Med Rec frequently asked questions (PDF 113.6 KB) for common misconceptions.
Sustain and spread
Once a change is in place and showing measurable improvement, the final step is to keep it going and extend it across the service.
Develop a sustainability plan early, not at the end of the project. Involve your QI advisor.
Embedding improvement into practice usually involves:
- standardising work processes, roles and responsibilities, and documentation
- folding Med Rec education and training into existing training for all clinicians involved in medication management
- continuing data collection and evaluation to monitor and refine the process.
Sustain measurement over time
Embed data collection into standard practice in your ward or health service. Include staff and patient stories and other feedback to track sustainability.
Once testing ends, you can collect data less often. For example, move from monthly to three-monthly collection, then to six-monthly. Make sure your project sponsor, health service executive or senior management can see this data.
If the improvement is not sustained
If compliance drops at any point, step back in. You may need to resume more frequent measurement to understand why and repeat your PDSA cycles to get the change back on track.
Useful frameworks include the National Health Service England Sustainability Model.
Spreading means actively rolling the change out to other wards, units, services or districts. What works in one setting may not work in another, so revisit the improvement process and adapt for local context.
Resources
Build the measures into your health service's performance indicators and run regular audits at a frequency the health service sets.
Healthcare doesn't stand still. Paper-based medication charts have given way to eMeds, and established processes will keep being challenged by new technology and changing practice. Regular monitoring is how the improvement keeps pace.