This page is for antimicrobial stewardship (AMS) pharmacists, infectious diseases physicians, clinical microbiologists, infection control practitioners and teams leading AMS improvement projects in NSW Health services.
This toolkit contains AMS-specific worked examples, templates and resources to plan, run and sustain a quality improvement (QI) project.
Register your project team to gain access to the Quality Improvement Data System (QIDS). Available to NSW Health staff only.
More about the approach underpinning this toolkit
Getting started
Set a realistic timeline before you start. Lasting change usually takes 6 to 18 months to test and embed. Expect less time if you've built on earlier improvement work, or more if the change is complex or spans multiple services.
Start by identifying a specific AMS problem at your facility. Common examples include:
- low concordance with surgical antibiotic prophylaxis guidelines
- poor documentation of indication, stop or review date, and antimicrobial allergies
- delayed IV to oral antibiotic switch when clinically safe.
At this stage, name the problem only. Do not propose solutions yet.
Improvement projects need a problem that people are motivated to solve. Common errors at this stage include:
- selecting a problem no one is interested in
- jumping to a solution before investigating the problem
- focusing on a process that is currently unstable (for example, a paper-to-electronic transition)
- choosing a problem outside your team's sphere of influence.
Assess your unit's readiness for change by reviewing existing culture, communication, team practices and safety and quality concerns. If there is significant resistance, address it before proceeding.
Gather local data to support the problem you have identified, using sources such as:
- national antimicrobial utilisation surveillance program for antimicrobial use data
- national antimicrobial prescribing survey (NAPS and Surgical NAPS) for point prevalence data on appropriateness
- incident management system for antimicrobial-related incidents
- resistance organism reports from your microbiology service
- clinical audits
- baseline audit: design your own using the Auditing surgical antibiotic prophylaxis (PDF 290.0 KB) fact sheet if existing data is insufficient
- gap analysis: use the Australian Commission on Safety and Quality in Health Care structure indicators for AMS programs
- staff and patient stories: qualitative insight that complements your numbers.
Seek guidance from your clinical governance unit, infectious diseases, pharmacy or infection control departments. You can also contact us for advice on sampling numbers and data sources.
The improvement project brief sets out the problem, why it matters, how long the work will take and the approach you will use. A strong brief is grounded in your data, takes sustainability into account, and aligns with your health service's priorities.
Use the brief to gain a project sponsor: someone in a senior position, ideally not working directly on the project, who has authority to remove barriers and secure resources. The level of seniority depends on the scope of your project (for example, a nurse unit manager versus an executive director). Communicate with your sponsor regularly.
A project charter example of promoting IV to oral antibiotic switch (PDF 296.9 KB).
Find a project sponsor early. Present your case for change and ask them to support the work.
A good sponsor:
- has authority to approve changes
- secures the resources the team needs
- helps remove barriers as they arise
- holds a senior role but does not work directly on the project
- believes the problem is worth solving
Communicate closely with your sponsor and provide regular updates. Your project sponsor can guide where governance sits within your health service. Operational responsibility usually integrates with existing meetings:
- Unit or ward level: Quality use of medicines review meetings or departmental meetings.
- Health service, local health district or speciality health network level: AMS, medication safety, or drug and therapeutics committee meetings.
Governance is separate from your project team. The project team carries out the interventions.
The project needs a multidisciplinary team with a team leader to steer it, and members committed to actively supporting it. QI projects often fail when team members lose interest or stop participating, leaving the leader to carry the work alone.
The project team's role is to:
- evaluate current medication reconciliation processes
- identify and enlist clinical champions
- set general goals
- develop, run and evaluate improvement strategies
- share results and findings.
Suggested team members
- team leader: the voice of the project, runs meetings and coordinates the work
- quality improvement advisor or expert
- AMS pharmacist
- infectious diseases physician
- clinical microbiologist
- infection control practitioner
- pharmacist, nurse unit manager and clinical nurse consultant from the targeted ward
- junior medical officer and medical consultant from the targeted specialty or team
- consumer representative: or use interviews or surveys to capture consumer perspectives.
Consider inviting colleagues likely to challenge the project. They often raise barriers and perspectives that strengthen the work.
Once the team is in place, align on the problem the project is targeting and what is in and out of scope. Without a well-defined scope, projects tend to grow beyond what is achievable, lose focus, and fail.
Making improvements
This stage moves your project from problem-definition into structured testing: writing an aim, mapping the current process, generating change ideas, and testing them in small cycles.
Your aim statement captures the goal of the project. It must address the problem and must not include a solution.
A SMART aim is specific, measurable, achievable, relevant and time bound. Remember:
- "some" or "better" is not a measure, and "soon" is not a time frame
- start small. Focus on a single unit or ward, even if the problem is widespread. Refining your approach on one unit gives you the evidence and confidence to spread the work
- avoid aim statements that suggest the desired solution, for example "implement a specific policy or process on your ward".
Examples:
- Within 12 months, 95% of prescriptions for surgical antibiotic prophylaxis for general surgery patients will be concordant with guidelines.
- By December [year], 95% of geriatric ward B patients labelled allergic to penicillin will have their allergy verified and validated.
- Within 6 months, 95% of antimicrobial orders in General ward C will document an indication.
- Within 9 months, at least 95% of inpatients under the care of general paediatric teams prescribed IV antibiotic therapy are switched to oral therapy within 24 hours where safe and appropriate.
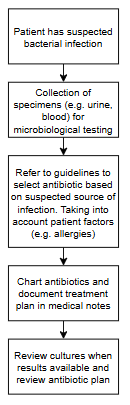
Develop a flow chart of your current AMS process with your team. Map each step and decision from the time a patient enters the ward or facility until they are discharged. The flow chart shows how the process actually happens, not how it should happen.
Use it to identify:
- the entire AMS process as it currently runs
- current roles and responsibilities for each step
- time-critical points, gaps, bottlenecks and variation
- where data may need to be collected to demonstrate reliability (for example, specimens collected for microbiology before antimicrobials are commenced).
Once you have identified gaps with baseline data, brainstorm why they exist. Without understanding all the causes, solutions may focus on the wrong part of the process and the problem continues. Use the 5Ws and 1H brainstorm method against the gaps in your flowchart.
Resources
{kind=link}
{kind=link}
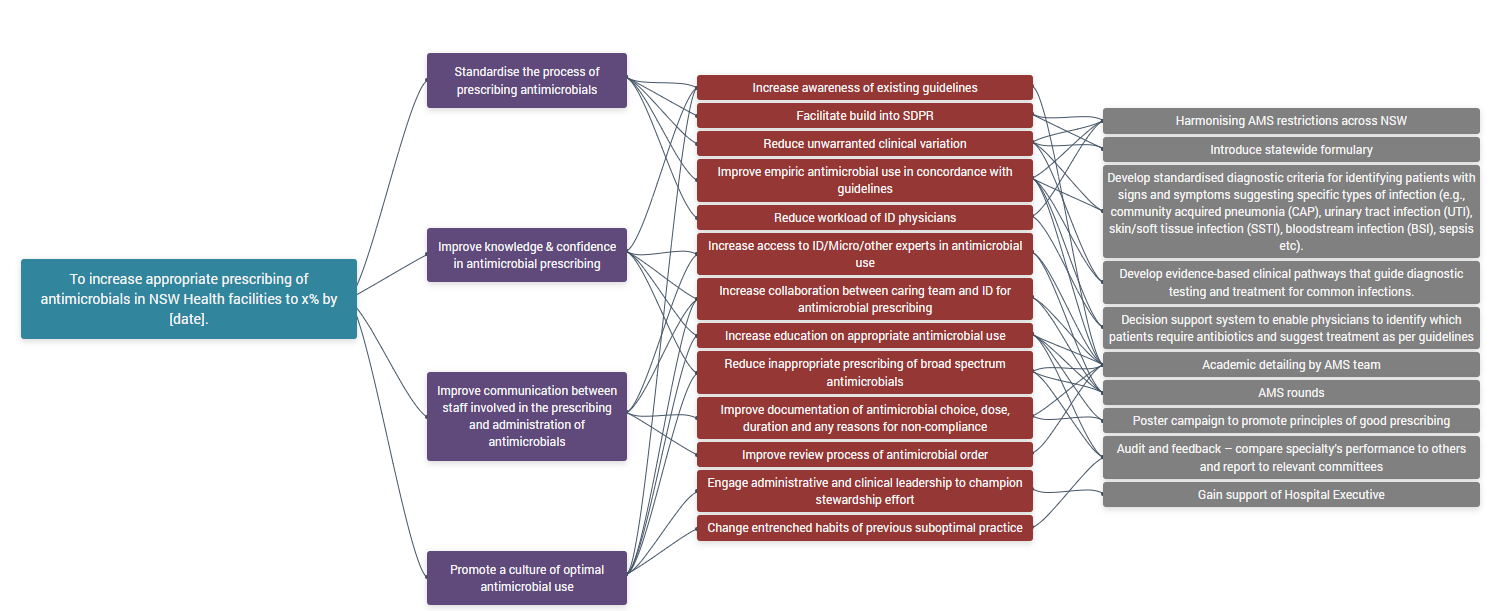
Sort the causes from your brainstorm into themes using an affinity diagram. Extend this into a driver diagram, which shows the relationship between your aim, the primary drivers (high-level factors that need to change to achieve the aim) and the secondary drivers (specific factors or interventions). Involve your QI advisor in this step.
Use the driver diagram to brainstorm change ideas for each secondary driver. Not all changes lead to improvement, so prioritise carefully. For each change idea, consider:
- how easy or hard it will be to implement (cost, time, training)
- the impact it will have on achieving the aim
- feasibility, logistics and expected outcomes.
Example: Replacing 1 g cefazolin vials in operating theatre imprest with 2 g vials is easy to execute and high impact, because it makes it simpler for clinicians to administer the correct 2 g dose for most patients (drawing from one vial instead of two). This is a strong early test in a SAP project.
Hard-to-implement changes should not automatically be deprioritised. Some of the hardest changes lead to the biggest improvements.
Resources
{kind=link}
{kind=link}
Plan, Do, Study, Act (PDSA) cycles test changes on a small scale before scaling up. Start with one patient, one shift or one team. If the test works, expand (for example, three patients, three shifts, three teams), then continue scaling up.
PDSA cycles are designed to be rapid and sequential. Implementation only happens once small-scale tests achieve a reliable improvement.
Tips for PDSA cycles in AMS:
- test no more than three change ideas at a time
- start scaling the next change idea once you are confident in the first
- monitor your measures continuously
- briefly document each cycle through all four stages.
Example PDSA, cefazolin vial change
| Plan | Change cefazolin 1 g vials to cefazolin 2 g vials in Operating Theatre (OT) imprest, starting with one theatre on a single elective list. Predict that the correct 2 g dose will be administered to patients without prompts. |
|---|---|
| Do | Remove cefazolin 1 g vials from imprest and replace stock with cefazolin 2 g vials. Inform all OT staff and anaesthetists of change. Provide education and resources on the correct dosing of cefazolin perioperatively. Observe the next 10 cases and note any feedback from OT staff. |
| Study | Compare the dose administered against approved guidelines. Document any issues with stock, wastage, delays in dosage or unexpected behaviour. |
| Act | If successful, expand scope to all theatres. Continue to collect data over several weeks. If any issues are identified, modify and re-test. |
Data for improvement
When you test change ideas, collect data in real time rather than retrospectively. Quantitative data will form the bulk of your measures, but qualitative data is equally valuable.
Resources
Choose your measures
A single measure is rarely enough to determine whether improvement has happened. It is important to define the numerator and denominator and provide an operational definition for each measure to ensure data consistency.
Include one or two measures from each of three family of measures.
Outcome measures outline how the overall process or system is performing.
Example: Percentage of eligible patients on IV antibiotics that are stopped or switched to oral therapy within 24 hours (target ≥ 95%).
- Numerator: number of patients changed to oral therapy within 24 hours.
- Denominator: number of eligible patients meeting criteria for a safe and appropriate switch.
- Operational: "Eligible patients" meet the criteria for a safe switch: clinically stable, able to tolerate oral medication, an appropriate oral antibiotic is available, patient likely to be adherent, and patient or carer agrees with the plan.
Process measures outline steps in the process performing as planned.
Example: Median time taken to switch eligible patients to oral antibiotics.
Balancing measures outline whether changes are causing problems elsewhere.
Example: Number of patients recommenced on IV antibiotics within 48 hours after oral switch.
Before collecting data:
- review existing baseline or historical data on the process you are improving
- collect baseline data for your chosen measures if needed
- agree as a team on who, when, where and how data will be collected
- find the most efficient way to access the data
- assign individual team members responsibility for each measure
- record data in QIDS (preferred) or a shared spreadsheet
- speak with staff and patients while testing to hear about their experience
- continue collecting data after the project to confirm gains are sustained.
Determine how much data to collect. Quality matters more than quantity. Ensure enough data is collected to determine whether the implemented changes lead to improvement. A data pool which is too small may not capture the effects of the change; conversely, a large pool of data may not possible due to time or resource constraints.
As a minimum, collect 5 to 10 data points each week (for example, 5 to 10 patients). Collect either consecutive cases or a random sample. Adjust based on the size of your service and the frequency of the problem.
People who can help with data collection
- health information data team
- ICT or eMeds team
- local clinical governance or patient safety team
- medical records
- pharmacy department
- executive sponsor.
Once data is collected, your team needs to interpret it to see if improvement has happened. Enter data into a spreadsheet or QIDS. QIDS builds charts directly from your data.
Run charts are line graphs showing data over time. They are an effective way to tell the project story and communicate progress to stakeholders. Annotate run charts to show when each change idea was tested and how it may have driven improvement. Your local QI advisor can help with displaying and analysing data.
To know if an improvement is real and lasting, look at patterns in your data over time. Probability-based rules help separate genuine change from random variation. On a run chart, for example, six consecutive data points above 95% signal a reliable improvement. This means the new process is followed 95% of the time.
See safety intelligence data tools for more options to present data, including histograms and control charts.
Once the change idea (or combination of ideas) is producing reliable improvement, begin your project evaluation.
Communicating change
Each group affected by your project will need different communication approaches. A stakeholder engagement plan sets out how you will communicate with patients, carers, clinicians, non-clinical staff and executives. It specifies the frequency, type and content of communications that build and maintain engagement at every level.
Each stakeholder group has different needs and motivations. Useful activities for AMS projects include:
- organising or participating in Antimicrobial Awareness Week, World Sepsis Day, AMS forums and similar events
- using hospital-wide channels (newsletter, intranet, memos. See surgical antibiotic prophylaxis page for correspondence templates
- promoting shared decision making with consumers
- using local nursing, medical, pharmacy, AMS, infectious diseases and infection control champions to advocate for improvement
- creating a ward display board or face-sheet handout with project data
- setting a standing agenda item or short presentation at regular meetings
- using double-staffing time or staff meetings for short, regular updates
- creating posters, lanyards and computer screensavers
- holding a project launch or workshop, or integrating engagement into existing events (medication safety forums, Grand Rounds)
- running a quiz, creating social media posts or sending email updates
- distributing information to general practice visiting medical officers in rural and regional areas.
See IV to oral antibiotic switch for posters and information for patients.
Providing education
Developing and delivering education is a fundamental component to ensuring project success. Education and training will need to be delivered to a variety of stakeholder groups at numerous points throughout the project lifecycle.
- Open with an interactive poll or pre- and post-quiz to check perception and knowledge change.
- Include a recent patient story from your health service to build engagement.
- Invite an AMS representative to speak to the targeted unit or ward.
- Keep sessions short and frequent; plan coverage for staff working after hours or on weekends.
- Collect attendance records and post-session feedback to improve future sessions.
- Share planning and delivery across the team, so no one person has to do it all.
Sustain and spread
Once a change has produced a measurable improvement, the final step is to embed it into everyday practice and spread it across the service.
Develop a sustainability plan early, not at the end of the project. Involve your QI advisor.
Embedding improvement into practice usually involves:
- standardisation: work processes, roles and responsibilities, documentation
- education: built into routine training for all staff
- ongoing measurement: collected and reviewed regularly.
Sustain measurement over time
Embed data collection into standard practice in your ward or health service. Include staff and patient stories and other feedback to track sustainability.
Once testing ends, you can collect data less often. For example, move from monthly to three-monthly collection, then to six-monthly. Make sure your project sponsor, health service executive or senior management can see this data.
If the improvement is not sustained
If compliance drops at any point, step back in. You may need to resume more frequent measurement to understand why and repeat your PDSA cycles to get the change back on track.
Useful frameworks include the National Health Service England Sustainability Model.
Spreading means actively rolling the change out to other wards, units, services or districts. What works in one setting may not work in another, so revisit the improvement process and adapt for local context.
The Institute for Healthcare Improvement’s seven spreadly sins (PDF 424.9 KB) sets out practical pitfalls to avoid.
Once an improvement is sustained and spread, the health service is responsible for ongoing monitoring. Build measures into your performance indicators and complete audits at a frequency determined locally.
As technology evolves, revisit the process to make sure improvements remain embedded.